
As regular readers know, I live in Ontario and because I have cancer (no worries, my odds of dying are about 2%) I’ve been in and out of the hospital system a lot from about 2018 to now.
That means I’ve gotten to see what happened to hospital care, albeit mostly in two hospitals; but two important, well funded research and teaching hospitals.
And it has been bad. Getting imaging tests which I would have had within a month to two before Covid took almost a year. A surgeon I know told me how he was fighting to get people urgent care. I’m lucky, I have a slow growing type of cancer, if I’d had something fast, odds are I’d be dead.
Diagnosing early is important for all sorts of diseases, not just cancer, and so is getting people quick care.
The union responsible for health care workers in Ontario (CUPE) put out a report on Ontario’s hospital care situation. I read it. It’s based entirely only publicly available numbers from various agencies like Statistics Canada, so even though CUPE has an obvious axe to grind I find the report accurate . And those numbers confirm what was obvious anecdotally.
(As an aside, the federal government gave Ontario billions of dollars to help with Covid which it did not spend on Covid.)
It starts with a section showing that Ontario has less health care workers (except research types) than other provinces. It’s not that they’re doing great, it’s that Ontario is worse and was even before Covid. It then shows how many vacancies there are:
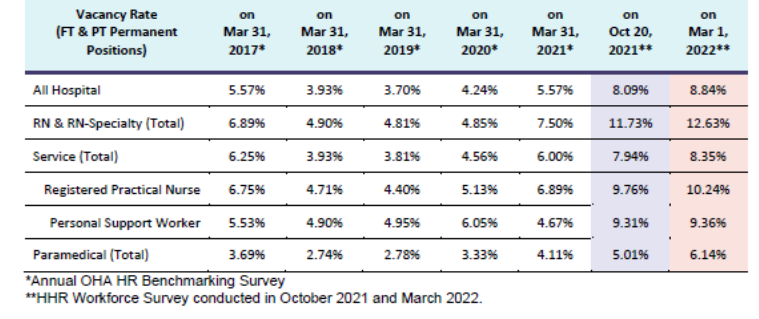
The effect of Covid is pretty clear.
We then move to the reduction in number of surgeries (but, alas, no report on imaging wait times.)
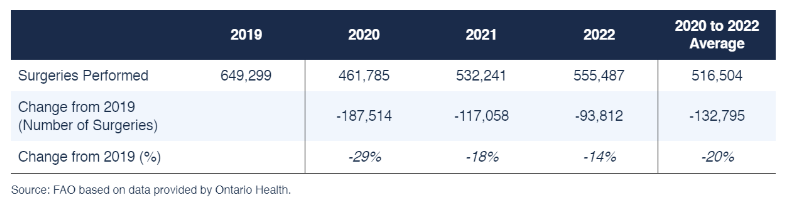
Given the population is increasing (massive immigration) and getting older this is pretty significant, and…
So, yeah, less surgeries, increased wait times and not just for elective surgeries. In visual format:
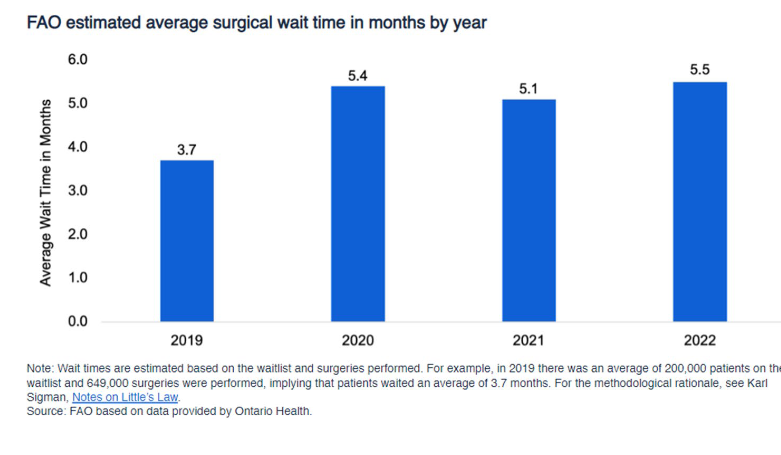
And….
So, what’s the government doing about this? I’ll just quote straight from the report (excuse the images, the report is a pdf and it’s easier to just show a picture.)
In other words, the government plan will make things worse. To keep service levels where they are (not to get back to pre-Covid levels) would require a little over 3,000 beds.
To go back to pre-Covid levels of care would require 8,170 beds over 4 years. The beds have to be staffed:
A 5.18% annual increase in staff means 13,986 extra staff added in the first year. (Assuming we start with 270,000 hospital staff). This would mean 60,000 extra hospital staff over 4 years (a 22.39% increase). This is not the number of staff that needed to be recruited, this is the number of extra staff needed to be added to the existing complement.
So, health care in Ontario hospitals, unless government changes course (they aren’t going to, at least not under this government) will keep getting worse, and it’s already bad in many ways (the actual care in the hospitals I go to is good, once you get past the wait times, though I haven’t been an in-patient since Covid started.)
CUPE has a bunch of other suggestions about how to fix this, you can read them all if you want, but I’ll highlight a couple:
Ban the use of nursing agency staff. These agencies charge 2x and 3x what hospitalspay their own staff, and they bleed away resources from round the clock and weekend staffing, worsening morale and weakening the continuity of care.
Real wages must increase. In any other labour market with skill shortages, wages would increase to retain and recruit. But real wages are being cut for Ontario’s health care workers and this policy is leading to an exodus of staff and to demoralization
There are about 15,000 licensed nurses who don’t practice in Ontario and thousands of frontline support staff have quit and to lure them back you’ll need to pay.
Anyway, what’s Ontario doing, in addition to not increasing beds enough? (If you guessed their non-solution starts with P, go to the front of the class.)
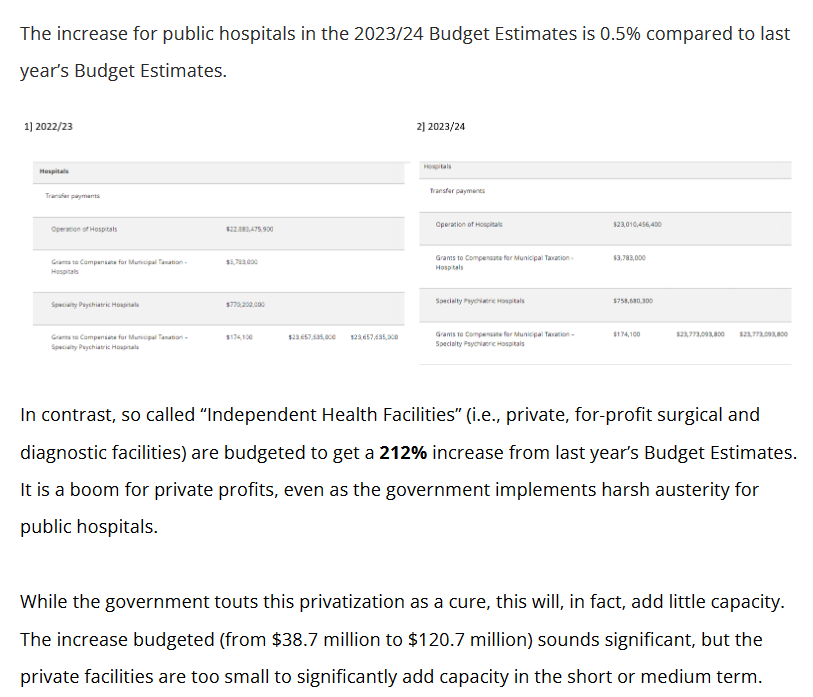
Now CUPE charming notes that the percentage increase is of such a small amount that it can’t fix the problem, but we all know that the real plan is simple: keep making public care shitty and eventually increase the private share massively, splitting the system into a shitty one that poor and middle class people have to use and a good system that the upper class and rich (and politicians who somehow get discounts) use.
The Ontario privatization plan is in its infancy, but the bones of it are clear. Get the people with power and influence to stop supporting public health care by letting them avoid its problems and get good care, make the care in the public system bad to make the mass population support privatization thinking they’ll get to use it when they really need it (as in the US, if you’re really sick and middle class or even lower upper class, you won’t be able to afford private health care), and eventually make politically connected friends very rich while destroying effective public health care.
You may be thinking “who cares what’s happening in a single Canadian province? I’m not Canadian, and don’t live in Ontario.”
But this is a general pattern. It’s happening in multiple countries including the UK (where it’s much further along), Canada, Australia and others. I highlight this one because of just how clear the report is, both on the effects of Covid and the longer term issues and because my personal experience supports it.
If you want good health care you have to pay for it. Public health care is cheaper than private (this isn’t even remotely in question, but beyond the scope of today’s post) and the only way to get good health care is if people are treated equally. If people with power or wealth can skip the queues and get better, faster care, then they don’t care what’s happening in the system you use and that system will get shit fast.
The first stage of privatization was creating a very tiny alternate system where the richest could get everything from private hospital care to bespoke MD care. I spent a tiny bit of time in that system around 2013/2014 and I can tell you, the care is better, by far. (Among other things, the doctor isn’t trying to rush you out of the office in fifteen minutes max and hoping for five minutes. I spent an hour and a half with a doctor during my first intake and often 30 minutes on other occasions. In the US they are offering two day complete check-ups seeing multiple specialists at a major hospital. Don’t worry, not 1-in-100 of my readers can afford that.)
Everyone gets treated the same for the same problem, or care will suck for everyone who isn’t powerful and rich.
As for Covid, we all knew it had a massive effect on the hospital system, and I guarantee that is true almost everywhere, not just in Ontario.
If you want good healthcare, the care the upper classes get can be no better than yours.
And Covid isn’t over and even if you never get it, it can still kill you, your kids, or someone you care about because they don’t get the care they need, when they need it.
(Read the full Ontariot Hospital Care report.)
Folks, it’s your donations and subscriptions which make it possible for me to keep writing (since I need to eat and pay rent and the cost of both have skyrocketed) so please (if you aren’t struggling) DONATE or SUBSCRIBE.
Willy
I think a significant percentage of the general population knows that wealthy PTB have been continuously pressuring the medical business to become a full-blown money extraction racket. Many can remember the days when that business used to be just a bit expensive, but within agreeably functional limits.
We just don’t know what to do about it. Besides wasting valuable bandwidth here complaining about it.
Feral Finster
Start liking it.
Richard Holsworth
Here’s former CIA agent and whistleblower Philip Agee outlining why the CIA has to destroy any alternative to Capitalism. pic.twitter.com/XnKkBVxsjG
Interesting and not surprising anyone who studies the machinations of capitalism come sto the same conclusion. You’re dead or your capitalist — nothing else will do. I googled the unrolling of Socialism in Scandinavia, or some such thing and was directed to the assassination of Olof Palme in 1986 he had been leading Sweden toward actual Socialism. He was killed a “botched“ investigation didn’t come to any conclusions. Yeah that’s what they do.
responseTwo
same thing is happening in all services in the capitalist west. they always want more money and will do whatever it takes to get it. all taxes go to war and making profit. capitalism will collapse from an overdose of greed.
VietnamVet
To be honest, the current system in the USA is approaching collapse. To make it worse, it is sanctioned eldercide – a combination of oligarch wealth extraction, disaster capitalism, and intentional ethnic conflict.
I am still here because I can isolate at home in suburbia and have not been transferred to an old soldiers’ home. But I have been forced back into the medical system and risky environments to get my medicine. Masking is so haphazard it is pointless. Nowhere is there clean filtered air. My replacement private eye doctor no longer accepts my Blue Cross Government Health Insurance and has yet to get my medications right. So, I’m back to going to the Veteran Affairs (VA) Eye Clinic to get my medications that I need to continue to see.
So far, I have driven back and forth without an accident (despite close calls) nor have caught a variant, by sheer luck.
Among the many lies and denials, the worse is ignoring COVID’s effect on competency. Good workers are necessary to keep society running. I got a huge water bill because of faucet leaks. My local plumber from before the pandemic who replaced the dishwasher and water heater did nothing in two visits and I gave him $200 because he brought his daughter along and said he has run out money. I took the gamble and replaced the stems myself and now just have a drip. I’ll see how much this cuts the bill. The only alternative is a hedge fund owned plumbing franchise.
It is a warzone that is very confounding because there is no shelling or a nuclear apocalypse yet. It is a silent conflict in the national capital region that is oblivious in the traffic jams without a competent government that serves the people.
someofparts
https://wendellpotter.substack.com/p/after-missing-mid-year-financial
That link takes you to Wendell Potter’s substack. Everything he posts about the US healthcare system is worth reading.
The specific post I linked to is about the things the health insurance criminals will be doing this year to make even more money, since Wall Street thinks they did not make enough last year.
Should I move to Mexico for the healthcare?
Carborundum
While I agree that the government’s not too subtle aim is to introduce two tier healthcare, what goes unstated here is how terribly healthcare is managed. MoH is an absolute shit show of vertical stovepipes, combined with multiple ingrained layers of agglomeration / “management” serially developed over multiple decades in the hopes that this time something will miraculously happen to make the system more responsive and accountable. I see (at least) three key drivers here:
1) MoH headcount is ridiculous (the common comparator is IIRC Sweden – last I heard, we were running 6X their headcount – with poorer outcomes).
2) Agglomeration of service delivery into large, centralized healthcare systems rather than the old more distributed norm of hospitals (or smaller multi-facility systems). The associated chicken and egg phenomena has been a massive increase in the number and influence of professional healthcare management types and their associated empire building.
3) Reflexive physician-centred rather than patient-centred norms / culture. If you’ve had to schedule multiple appointments on multiple days to work through a progression of tests and consults that we know based on the medical condition to usually be associated, you’ve lived this.
For bonus points one could also point out that we’ve yet to see real acknowledgement that when one is fighting the healthcare battle so predominantly in hospitals / acute care, one is already fighting at a significant disadvantage. Study after study has shown hugely significant multipliers on spending in areas like preventive medicine, public health, determinants of health, etc. but we keep throwing cash predominantly at the cost drivers at the expense of much more modest investments that would help us reduce demand.
Ian Welsh
Carborundum,
I was curious what you’d say. Without looking into it more right now (though I will in the future) I’d be very surprised if the staffing ratio issue is not admin bloat related. Dealing with that is something I’m very interested in, and it goes far beyond MoH (academia is another place where it’s ludicrously out of control.)
What I can say for sure is that I’m seeing the effects on the front line, and the stats on surgeries suggest that while anecdote isn’t stats, the stats support that. (Given I’m in Toronto and have cancer, I’m sure you know which hospital I deal most with.)
Also people like to confide in me, so I hear things from the staff. Anecdote, but… consistent.
As for the non-hospital workers, no question that’s an issue. But right now what I’m seeing is the government just doesn’t want to spend the money either way, unless it helps privatize. Hell, they refuse to even spend the money the Feds gave them for Covid on healthcare.
the pair
it’s happening in MAGAlberta as well. ever since the lunatic freak smith came in she’s been intent on pouring gasoline on the fire. one clinic pulled a “private care for VIP oil scum” stunt and it was only public shaming in the media that resulted in any punishment. a private testing chain was given significant chunks of the lab business and they f’ed it up royally resulting in 4 hour waits and dropped appointments.
i started “getting” it in 2000 when bush jr “won”: it’s a massive mistake letting conservatives into government when they openly state their delsuional ayn rand/milton friedman beliefs that ANY state power over ANYTHING is communist evil. it’s like letting a KKK grand wizard run the NAACP (not that he’d do much worse than their current leadership but the point stands). let ford and his handlers have a choice: go p_ss off to galt’s gulch and let society fucntion or get their brains taxed out to fix the mess they’ve caused.