
So, I see today that Democrat Tammy Baldwin has endorsed doing a Medicare buy-in starting at age 50.
Which means that access to good health care will remain age- and money-gated. If you’re too young and too poor, you don’t get health care, or you get worse health care.
Here’s the simple rule for a good healthcare system: The health care someone gets is based only on what they need and not on ANY other consideration.
This means everyone is treated the same. If society decides that some treatments are too expensive, then the criteria used for whether you get them is never “Can you pay?” it is criteria like “Who will this help most, medically?”
Of course, it is impossible to deal with America’s healthcare mess without also dealing with oligopoly device and medicine providers.
That means you must either regulate them (“You will make a 5 percent profit, no more and no less”) or you must break them up, or you must nationalize them.
When the price of insulin has risen like this…
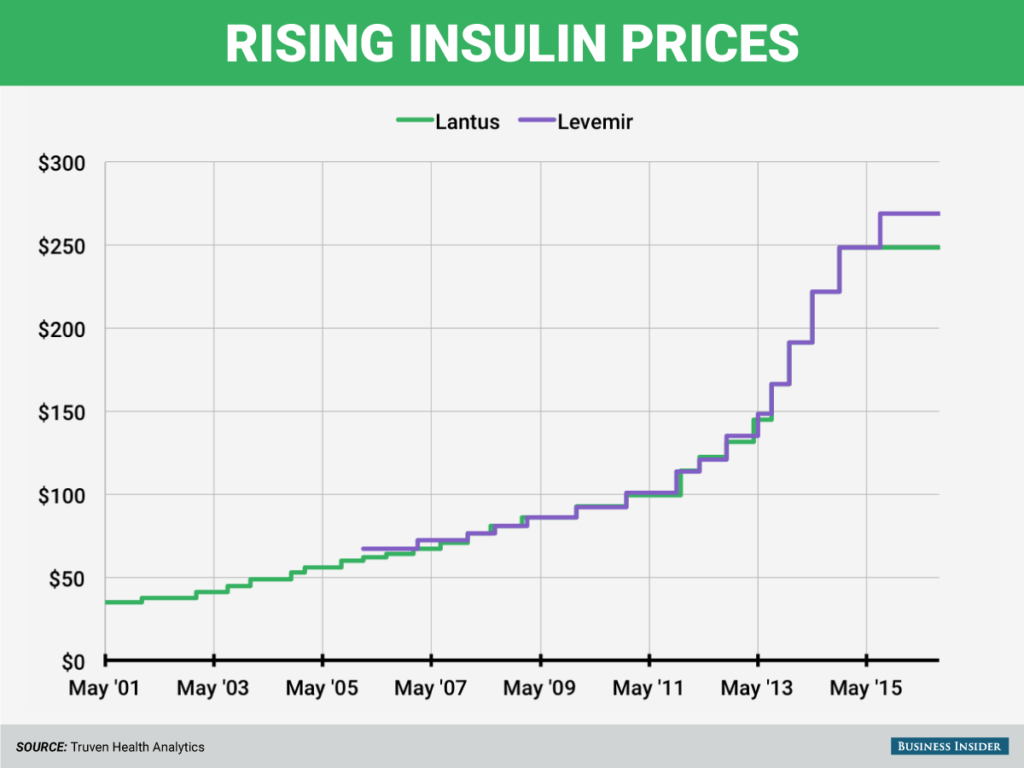
… you know that the market has failed. And this is for a drug that is not patented.
A few people are getting very rich, by killing people. Those people should have their companies expropriated for nothing, and then, if any charge can be found, criminal proceedings should ensue. At the least, they should be made pariahs, and anyone who deals with them in any way should be ostracized.
But, moving back to policy, if you just give everyone health care, stop rationing based on money and age, and break the oligopolies (while fixing various other perverse incentives like doctors owning testing companies), not only will the cost of healthcare plummet (Canada’s per capita costs dropped by a third in ten years just by changing to universal care), its quality will increase.
But I still want to see most pharmacare executives in prison.
The results of the work I do, like this article, are free, but food isn’t, so if you value my work, please DONATE or SUBSCRIBE.
ponderer
Wow, I never thought I’d get to the age where I could get something at the expense of the next generation. I feel like a baby boomer! /s
Seriously, the medicare-for-all folks should build a list of penalties that ratchet up over time as it gets delayed. Turn the profiteers against each other using the same psychological FUD techniques the elites employee against the 99%. Taxes on wealth earned in certain industries over a certain time period above a certain amount. Better yet, Taxes on all the super rich that adjust based on time. A financial justification should be pretty easy, budget’s got to be balanced and all that.
StewartM
So, I see today that Democrat Tammy Baldwin has endorsed doing a Medicare buy-in starting at age 50.
Why this criteria, even from a $ perspective? Medicare and Medicaid already cover the oldest and sickest patients, adding bunches of younger/healthier patients don’t add much to the overall utilization of medical resources. In fact, the elimination of whole unnecessary bureaucracies involved in administration, bill collections, and whanot plus driving down the prices of care and drugs should mean that we spend far less money.
Willy
The entire health insurance, health care, pharma and lobby industries have contracted the rent-seeking virus. Major surgery is needed, stat.
HomoSapiensWannaBe
“Here’s the simple rule for a good healthcare system: what health care someone gets is based only on what they need and not on ANY other consideration.”
Ian,
This blanket assertion doesn’t take into account how much a person has taken care of themselves. Many, if not most, bad health outcomes, especially chronic health problems, are directly due to bad lifestyle choices. Granted, as children and teenagers, their parents/guardians are more responsible, but for adults? Sure, some bad outcomes are due to genetics and/or uncontrollable environmental factors.
Some, but not all, of the high cost of U.S. “sickcare” compared to other nations is due to the poor health of so much of the population.
Then, there is the negative health drag of living in such an economically unequal system, even for the the relatively well to do. However, the stress of it affects the less well off the most.
We need a better mix of social & private in our economy. There is so much unproductive capital and excess capacity in the system, yet most can barely make it to the next paycheck.
Overpriced credit for those who need it most is also a big part of the problem.
StewartM
HomosapiensWannabe:
Some, but not all, of the high cost of U.S. “sickcare” compared to other nations is due to the poor health of so much of the population.
Actually, from what I’ve read, not true. The US loses in mortality/morbidity comparisons with developed countries who have higher rates of smoking, heavy drinking, and equal rates of obesity (a lot of Brits seem to think we’re health nuts, from what I’ve heard). At most ‘healthy living’ makes only the smallest of dents in the overall stats (though I do think that Americans being overworked, sleep-deprived, and not having work leave like other developed countries is probably a significant factor; of course, being worked all the time–if you have a job–means you eat more junk food, don’t exercise enough, and don’t get enough sleep, so these correlate).
But I can’t help but to think the biggest reason we lose is that they get ready access to cheap or free health care, and we don’t.
About 20 years ago, I came across an accident scene, with two young adults seriously hurt (with apparently concussions to them both). When the young man was roused, he refused to get into the ambulance–because he couldn’t afford the price of the ambulance nor care. Now multiply such events where people should go seek care, but don’t because of cost, per lifetime and think of what the likely results will be across the whole US population.
metamars
“That means you must either regulate them “you will make a 5% profit, no more and no less” or you must break them up, or you must nationalize them.”
I’m basically good with this. I’d think you’d want to relax profit ceilings for new drugs or treatments, at least until R&D costs are met (or some reasonable multiple of that figure).
However, I don’t think this is sufficiently outside the current corrupt paradigm. (Which I personally don’t identify with capitalism, but rather unregulated capitalism, which is not fully subjected to human values).
IMNSHO, the government should be pursuing optimal healthcare approaches, and also aiming for the most bang for the buck, where interventions other than prevention are needed.
In the case of a need for insulin for type II diabetics, there are ways to increase insulin sensitivity (so you need less supplemental insulin, or even none at all) that most of the public doesn’t know about. Why is the government not educating the public, on a continual basis, about this knowledge? (If you don’t believe this, see, e.g., this video: http://www.buttermakesyourpantsfalloff.com/fasting-and-fifty-percent-insulin-problem/ ) Why does the government not forcefully include this knowledge as part of the educational curiculum, say grades 3-12?
Also, I’m sick and tired of hearing the excuse that “you can’t patent this, so no company will pay for FDA approval”. OK, fine, but the us government has deeper pockets than any corporation. So, e.g., as I wrote a while back on this website, near infrared light has successfully treated people with end stage kidney disease. So, why isn’t the government a) doing large scale tests, to prove (or disprove, as the case may be) these claims and b) if the claims are successfully demonstrated, educating the public to DEMAND such far, far cheaper alternatives than dialysis?
I’ve recently found out about seemingly highly credible anecdotal claims of cures of end stage kidney disease using structured water (technically, H3O2). Why isn’t the government similarly funding any and all tests to establish the statistical truth or falsity of these claims; and then educating the public about this far cheaper option, if the claims are upheld??? Making structured water is also going to be pennies on the dollar, compared to the million dollars per year, or thereabouts, of dialysis. Also, like the near infrared treatments, the quality of life is going to be so much higher.
(These claims were made by the “go to guy” for structured water research, Gerald Pollack, in this youtube video: “Dr. Gerald Pollack On How to Create The Perfect Water for Optimal Health” @ https://www.youtube.com/watch?v=2edKFnVX5CE&t=1957s
Starting at 31:38, running to 32:33 :
Pollack: I’ve seen cases where absolutely it can reverse pathologies, and what one was where, a guy called me 4 years ago, and he started tellingme about the water where the family is is drinking, where she had learned about it in a laboratory in which she worked. And you know she said I never have the flu or anything, anymore. Now OK, big deal. Then he said one of the neighbors knows somebody who had irreversible kidney pathology. And she was on dialysis and waiting for a transplant. And she thought “hey, can I try some of this stuff”? So she tried it and he told me that BY THE END OF THE MONTH she went from irreversible pathology to no pathology. So my response was “I don’t believe you”. Actually I did. but so he sent me the hospital records Um, so I’ve seen hospital records of many more people like that and a colleague friend of mine went to visit and interviewed the people who he claimed had been cured and he confirmed it. )
I recently stumbled into the following, which reveals the identity of one of the kidney patients that Pollack was talking about:
http://projectcamelotportal.com/2014/06/05/revised-interview-water-h3o2-with-black-project-scientist-rerecorded/ .
Isn’t it ‘funny’ that, while you used to be able to obtain the same structured water that this guy, Jef Harvey used (because he himself was selling it and/or a commercial grade device to make it), this guy died soon after the above interview, for “sudden, non medical” reasons (unspecified; see https://wakeup-world.com/2015/09/11/29-holistic-doctors-health-practitioners-poisoned-during-conference-critical-condition/) and the ball has been completely dropped? AFAICT, his company, like his website (jeftech.net) are kaput.
Where is the government in all this?? Not being proactive in facilitating low cost treatments, that’s for sure! I don’t mind the government limiting profits for dialysis companies and doctors, but that is a poor substitute for a more proactive approach. BOTH approaches should be used.
Of course, we all know the underlying cause for this – inverted totalitarianism, as Chris Hedges likes to remind us. The legalized greed of the current system is appalling, and morally indefensible.
The activists should be rousing the public, not just towards more affordable insulin and dialysis, but to alternatives that obviate the need for those things, at all.
Hugh
“Many, if not most, bad health outcomes, especially chronic health problems, are directly due to bad lifestyle choices.”
I agree completely with this. There are a lot of lazy people in this country who make bad life choices like being born into poverty, having no hope, choosing not to have access to a top notch education, or a good paying job, and, slackers that they are, sometimes no job at all, and not having a good background in nutrition, physical training, and medicine. And don’t get me started on all those people who choose really crummy genes.
I haven’t heard this “worthiness” argument in years. The primary problem with it is that we already have such a system, and it writes off the lower 80% of us on a regular basis. Worthiness is just another way for the rich and elites to shift the onus for something else off them and on to us. It’s our fault that they deprive us of the means and knowledge for a healthy and meaningful life. Shame on us! Didn’t we know, didn’t we realize? we were born unworthy.
As I have written and will continue to write, society is mother, father, sister, brother to us all. Without society, most of us would not exist, and those few who did exist which was both brutish and short. We get 99.99% of who and what we are from our society, right down to our language and religion or ethics. We have duties and obligations to each other, and primary among these is to provide the basics for a meaningful life to each and every of our society’s members. Healthcare is certainly one of these basics. If you want people to make informed decisions, then inform them, but make sure they have the basics to make these decisions real. I have had enough of the “keep them poor and ignorant but blame them for their choices” argument. We owe each other better than that. And some people will make bad decisions anyway. I think that’s called being human. We can do what we can to reduce these, or at least their effects, but it is no reason to tell people to just go die in a ditch.
Hugh
“and those few who did exist would have an existence which was both brutish and short.”
Donna Curtis
Preach it Hugh!
That &%$#@& above is going to get sick one day. He can blame himself for it if he wants but I’m going to try… just try… to enlighten him a little.
This is how it can happen to you to: I was in great health. Started dancing when I was three and was still teaching dancing part time before I got sick. At 47 I could still do a backbend even after a partial hysterectomy that required a vertical cut from my belly button to my pubic bone. I’d like to see you pull something like that off pal.
At 49 I was diagnosed with multiple sclerosis. No one knows why it happened. Long story short; unable to move around I began to gain weight. The coup de gras was a drug used for nerve pain with a major side effect of weight gain.
It was then that the really bad genes in my family kicked in and I got diabetes. About the best I can say is that I held it off for a decade longer than anyone else in my family.
So, mister HomoSapiensWannaBe, you’re just going to have to admit you are actually human like the rest of us and, therefore, not in perfect health ever.
Willy
Maybe the good health is trickling down from our betters and it just hasn’t gotten to us yet?
Back then, President Eisenhower warned about the military-industrial complex. And Walter Cronkite only reported “the way it is”.
Today, presidential candidate Ben Carson doesn’t say squat about the insurance-pharma complex, but he did lie about peddling Mannatech’s crapweasel pill products. And newsman Alex Jones sells his Super Male Vitality (with X-2 Combo) in a 5 pack for only $262 if you order today.
Somehow, things are different now.
Ché Pasa
Patient selectivity, race and class discrimination, and limits on access to health care services have been built in to the US system from the beginning. There’s no objective reason why we can’t have decent universal health care at a reasonable — if not necessarily cheap — cost, but American Exceptionalism is rears its ugly head to maintain regressive status quo.
I’m old enough to remember when what was an inadequate health care system was transformed into a sometimes deliberately cruel money-printing system for the benefit of investors and administrators.
Previously doctors were considered the primary drivers of high medical costs. Their fees and pay was considered outrageous — compared to that of most of their patients, at any rate. Controlling physician compensation and fees became a mission for some health care reformers in the post-War era. Otherwise, the general belief was that expanding health care access was important for the health of the nation.
That began to change in the early 1960s when administrators, many of them recent business school graduates, began taking over hospitals and running them for profit whether they were set up as non-profit entities or not.
Gradually, doctors were overridden and their pay was controlled (except when they owned the hospitals and clinics); administrators became the key employees (and sometimes owners) and costs began an inexorable rise into the stratosphere. The establishment of Medicare and later Medicaid contributed to this transformation, but it had been underway prior to their existence.
Today, for many patients, the US health care system is a nightmare. For many others, it’s not. It’s fine. Part of the nightmare is due to over administration of the system, layers and layers and layers of administrators whose primary purpose seems to be maintaining and enhancing profit on behalf of the investor/owner class, bugger the patient. As long as sufficient profit from the patient can be assured, they can get decent treatment most of the time.
Not enough profit? Tough luck, sucker!
Of course there have always been race and class barriers within the system, barriers which are enhanced by intricate administrative rules, flow charts, outcome expectations and so on.
None of this is a law of nature. It’s the way things have developed in order to protect the interests of the most powerful players in the health care industry. Breaking their power is the key to correcting the problem.
Don’t get me started on pharmaceuticals.
metamars
@Donna Curtis
“It was then that the really bad genes in my family kicked in and I got diabetes. ”
No, you’ve got that wrong, assuming you mean type II diabetes. You are being victimized by a bad and corrupt system, but part of that victimization has to do with you internalizing false notions held dear by the medical community. There is more than corruption going on, here – part is institutional inertia, reflecting human tribalism and irrationality.
I suggest you educate yourself about epigenetics. Not to mention holistic approaches to diabetes, in particular intermittent fasting, low carb moderate protein/high fat diet, etc. (A good place to start is probably “Fat for Fuel”, by Dr. Mercola, though I’m doubtful that one has to be so diligent about measuring biomarkers for ketosis, if you simply follow his dietary prescriptions. See also numerous free youtube talks and interviews of Dr. Jason Fung.)
Besides you doubtless having insulin insensitivity, your leptin is probably disregulated, also. Please take a look at “Epi-paleo Rx: The Prescription for Disease Reversal and Optimal Health” by Dr. Jack Kruse, who dropped about 130 pounds in a year, with no exercize and eating more than before.
Kruse is the most unorthodox guy I’ve ever encountered. I think he’s 90% genius, and 10% insane. Some of the things he says, regarding physics, are wrong, but I’m not sure if he’s just being very sloppy (kind of like Trump), or just making stuff up (kind of like Trump).
Regardless, his core belief about the centrality of healthy mitochondria is doubtless correct. An excellent interview which covers slam dunk evidence (only a few years old) that cancer is more a mitochondrial disease, than one of genetic mutations in cell nuclei, is here: https://www.youtube.com/watch?v=DaCZ3ivhwUY
Although it’s mostly over my head, and I’ll guess over yours, as well, this youtube gets into nitty gritty evidence of mitochondrial dysfunction behind a number of major, chronic illnesses https://www.youtube.com/watch?v=xDDFV7Sovvs&t=2102s . Your cellular genetics helps determine which particular disease develops, first, AFTER the mitochondria go awry.
If you want to blame your genes, you should at least blame your mitochondrial genes, first, not your cell nuclear genes. 🙂
metamars
“An excellent interview which covers slam dunk evidence (only a few years old) that cancer is more a mitochondrial disease, than one of genetic mutations in cell nuclei, is here: https://www.youtube.com/watch?v=DaCZ3ivhwUY”
Correction. The experimental basis for preferring the metabolic/mitochondrial theory of cancer vs. a cellular genetic basis, goes back decades. But the slam dunk, summary re-evaluation by Seyfried is relatively recent.
Hugh
Cancer involves a series of mutations where cells first ‘immortalize’. This results in local tumors. They then lose surface proteins which hold them to similar cells. This allows them to move about the body through the lymphatics and bloodstream. Finally, they have to express new surface proteins which allow them to be recognized by and taken up other organs (metastasis). None of this has to do with mitochondria.
I used to talk about universal single payer but as Medicare for All became more popular I switched to using this term. But it has an essential weakness which we now see more and more. It is very difficult to finesse “universal single payer” into something other than what it is. This is not true with Medicare for All. The gold standard for Medicare for All is probably the Conyers House bill HRH 676. It is universal single payer and, my understanding, takes most or all the for-profits out of the healthcare system. Sanders’ Medicare for All is universal single payer but leaves the for-profits in. Others use Medicare for All to mean another nebulous version of the infamous “public option” which Obama and the Democrats cynically used to suppress progressive opposition to the ACA. For those who don’t remember, the public option started out as an insurance option that was never defined and whose coverage progressively decreased from maybe everyone, to tens of millions, to a few million, to nobody when Obama dumped it. The Baldwin buy-in sounds very pragmatic to me. Pragmatic being code for giving the rubes crumbs and calling it a five course dinner.
Spring Texan
On pharma, Sanders has been highlighting this obscene reality: https://www.statnews.com/2018/12/13/catalyst-pharma-drug-price/ “An old, formerly inexpensive drug called Firdapse was just slapped with a steep new price tag: $375,000. The Food and Drug Administration approved Firdapse late last month to treat a rare, neuromuscular disorder called Lambert-Eaton myasthenic syndrome. Although it’s the first approved therapy for this disease in the U.S., there’s a catch: For years, hundreds of patients have been receiving an unapproved version of this drug for free.”
The company that used to provide the drug for free is now prohibited from doing so by our patent laws and many patients now pay thousands of dollars a month even if insured.
There is no limit to pharma criminality.
metamars
@hugh “Cancer involves a series of mutations where cells first ‘immortalize’.”
I suggest you listen to the Seyfried Mercola interview. You are describing a downstream epiphenomenon.
Will
I almost didn’t read the comments…. things have been so ~ahem~ out of sorts around here lately that I was afraid of what I’d see. I am pleasantly surprised. Good thoughts and I enjoyed reading them.
This is a discussion that desperately needs to be had. From coffee shops and lunch breaks to the highest levels of government. It is still early in the thread but I send a hat tip to all the thoughtful commenters.
Will
Mandos
The quacky woo is strong today in the comments. “Structured” water, argh. Next we’re going to get links to that awful Health Ranger guy, we’ve already descended to links from Mercola so why not dig deeper?
ponderer
@StewartM
“Why this criteria, even from a $ perspective? ”
To stall progress. The same way Obamacare could stall Medicare for All, then get turned back later. They know once Medicare-for-All happens and the insurance industry is decimated there won’t be an easy way to get it back because those lobby dollars are gone. They will delay as long as they can. They being the insurers and our corrupt political apparatchiks.
Willy
There’s nothing wrong with alternatives, as long as they’re proven to work. But since science is wrong and evil for killing God, the scientific method should be replaced with one involving religious practices. For now, I’m declaring that people get sick because they’re not eating kosher. Plus I overcame my cold faster by wearing a payot and shtreimel. You can buy a set online, but avoid the poor quality costume version. And never wear these with a low quality Harden beard. You might get beat up.
DMC
http://americanloons.blogspot.com/search?q=Mercola
Who needs government healthcare when there’s YouTube?
hotgingerbread
So the price of insulin went from $75 to $250 under Obama. The Dems are now the pro-war party, and have revived Russian scaremongering. I love me some lesser of two evils! Anyways, keep voting Democrats in, I\’m sure they\’ll save America, they\’re such lovely less evil people.
metamars
@DMC
You are apparently not only misinformed about alternative treatments, but also misinformed about orthodox medicine.
Orthodox medicine in the US is good at emergency care and some cutting edge interventions, but truly sucks when it comes to dealing with chronic diseases.
You can try reading “Don’t Let Your Doctor Kill You: How to Beat Physician Arrogance, Corporate Greed and a Broken System” by Erika Schwartz M.D., to get a clue.
The Bredesen protocol, an example of “functional medicine”, has reversed Alzheimer’s disease. I can’t remember the numbers, but I think it’s something like MOST of the patients Bredesen treated. Compare that with orthodox medicine….
More on iatrogenic illness @ https://www.sustainablemedicine.org/un-sustainable-medicine/death-by-medicine-iatrogenic-illness/
jrkrideau
@ Willy February 13, 2019
I’m declaring that people get sick because they’re not eating kosher.
Don’t be silly. People get sick because they are not eating an halal, ketogenic diet.
I am sure that Steve Mercola supports me on this scienificy proven fact.
Oh well, must rush, off to my reiki treatment.
Joan
I really hope a universal single-payer program can be implemented in the US. I’ve had friends tell me versions of “If I’m ever in desperate need of medical attention, don’t call 911.” When medical treatment is akin to financial suicide, it’s easy to see how people can become afraid of the system.
On the other hand, since the US has been cut off from its home remedy traditions for at least two generations, there are no alternatives that can be universally trusted. Pretty much all of alternative medicine comes off as fake. I’ve spoken with people who tend herb gardens and manage their health completely on their own. If I could convince my herb garden to do more than make of a cup of tea, maybe I would feel safer about being cut off from access to healthcare in the US. As it stands, my options are no healthcare, or paying money every month for no healthcare. I hope this changes for the better.
Joe
I find it axiomatic that if you show me a YouTube video, whatever you’re pointing me to is intellectual garbage at best, and dangerous misinformation at worst.
YouTube is a terrible thing, it’s catnip for loonies.
nihil obstet
I’d like a VA or NHS style system. Medicare for All retains the fee for service model, which requires lots of regulation to avoid perverse incentives. And I notice that veterans fight hard against converting the VA to a private voucher system; their experience is that the professionals do a better job when they’re not also profit seekers.
The political problems we have are the power of the medical and insurance industries, the entrenched belief in change by wonky tweaks, the belief in rational economic man who needs a price placed on anything to guide decisions, and the moralism we’ve seen here that we should only heal the deserving sick.
StewartM
Nihil Obstet:
I’d like a VA or NHS style system. Medicare for All retains the fee for service model, which requires lots of regulation to avoid perverse incentives. And I notice that veterans fight hard against converting the VA to a private voucher system; their experience is that the professionals do a better job when they’re not also profit seekers.
The VA wins as the ‘best health care in America’ award:
https://washingtonmonthly.com/magazine/junejulyaugust-2017/the-best-health-care-money-cant-buy/
That being said, I don’t see this is an either/or, why not both? Expand the VA to be full-access for everyone, build or buy clinics all across the US in every community (especially with an eye for access for low-income people). Allow people who wish to seek private health care hospitals and clinics instead, but use the VA’s pricing to set the reimbursement rates for treatment, with the stipulation that the private provider cannot deny anyone care and moreover the patient cannot be charged anything in addition to the reimbursement. The government would then not care if you went to the VA or to a private provider, as it would cost the government the same.
This would, I believe, drive for-profit medicine out of existence (a good thing, IMHO) and we’d be left with a public system plus a private system run by churches, humanitarian groups, and other non-profits.
Mark Pontin
Ian wrote: \’This means everyone is treated the same. If society decides that some treatments are too expensive, then the criteria used for whether you get them is never “can you pay”, it is criteria like “who will this help most, medically.”\’
It\’s an admirably succinct post you\’ve written here, Ian. Ten years ago — in a society that wasn\’t run by sociopaths — yours would be the the simple, practical criteria for what a decent, ethical healthcare system should look like.
Today, it\’s becoming increasingly impractical, even without reference to the sociopaths.
For merely one single instance of why, consider the case that was recently in the news of the Chinese scientist He and his CRISPr-enabled gene-editing of a human baby so that HIV susceptibility was removed.
To be clear, the Chinese have a real, growing problem with AIDS —
\’The growing threat of China\’s HIV epidemic\’
https://www.thelancet.com/journals/lanpub/article/PIIS2468-2667(18)30098-7/fulltext
Indeed, the Lancet link possibly lowballs the numbers. Nobody in China is going on the record yet, but if you talk to Chinese healthcare people and those over here who are familiar with their system, the emerging mind-set over there is that their population is so large that to attempt to treat HIVS using the expensive drug-based treatments that the West employs isn\’t feasible and, anyway, is less humane and efficient than simply erasing it.
By gene-editing it out of the population over the next couple of decades.
(And for those who believe the Chinese establishment\’s current line to the rest of the world, which is that He was just a renegade, please explain how He was brought back from Stanford and given a staff of 200 to work with.)
To be sure, Ian, China\’s gene-editing approach to HIV could meet your criteria of what an ethical healthcare system that treated everybody the same would look like. Arguably, it _is_ more humane and efficient to just _end_ human susceptibility to AIDS and the attendant suffering, rather than pootle around with drug treatments.
Nevertheless, look at what we\’re talking about if the Chinese proceed along this path: human speciation, if in a minor way.
He \’s gene-edited baby is only as a single example of what\’s coming. A tidal wave of biogenetic technologies are sweeping our way. Different societies and different individuals are going to make different choices about these technologies. Certainly, lots of people in the West are going to reject them. Particularly, Mercola-quoting naturopaths, Christian scientists, and fundamentalists of all stripes will simply want these possibilities legislated out of existence, though they won\’t be successful. Off the top of my head, a couple of technologies that are bound to have serious impacts are: –
In vitro gametogenesis: This will be sold as as a reproductive technology like IVF first, but is basically the capability to take any cell of somebody\’s body — including a hair or skin cell — and clone the whole physical individual. This technology exists _now_ in the laboratory. More here –
\’Disruptive reproductive technologies\’
http://stm.sciencemag.org/content/9/372/eaag2959
At least one team is shopping around among VC firms to commercialize it for fertility treatment purposes _within the decade_. Besides the fertility/reproductive angle, furthermore, in vitro gametogenesis has implications for designer babies – why fiddle around with messily editing embryos like He did with his attendant failure rate, when you can directly manipulate the cells from the beginning? – as well as for regenerative medicine. Which brings us to —
Synthetic organogenesis: Basically regenerative medicine, or growing new organs – hearts, kidneys, livers, epidermises, vaginas, penises, or whatever (different organs present different levels of complexity to be surmounted). There are, at any rate, four technological paths (that I know of) to growing new organs. Hence, one way or another there’s probably going to be an upsurge in the percentage of the global population aged 80-120 in two-three decades.
There are other disruptive biogenetic technologies out there. Let me conclude: in this world that’s coming, a baseline NHS or VA-style approach that offers certain basic treatments is desirable, but overall it will neither be practical nor desirable to have a healthcare system that “treats everyone the same” because: –
[1] People simply won’t want to be treated the same. If we have the vaxxers and Christian scientists now, what will it be like when the most effective treatments involve gene-editing and potential human speciation?
[2] As with China’s rejection of drug-based Western-style HIV treatment as impractical given their population size (if that’s the choice China makes), some regenerative medical treatments simply will be so expensive that they’re impractical for mass use, at least initially.
Here, capitalism could even be useful, in that a diversity of companies offering different regenerative medical approaches would play out with early investors in a given regenerative medical technology (aka longevity treatment) also being early adopters. Some early investor/adopters in some technologies could then die horribly as a result of their treatments; those in other technologies could live to 120. Thereby, a wide range of possibilities would be tried and the successful medical technologies selected for, and receive further investment and, quite likely, become cheaper and more accessible as a result. The history of cataract surgery is instructive in how a once-expensive treatment opposed by much of the medical community can in time become the easiest, most commonly-performed surgery in the developed world.
[3] Overall, in a very practical sense a Darwinian approach of having a diversity of technologies tried and selected from is more desirable than “treating everybody the same.” We’re talking about technologies whose implications may include human speciation, after all, so the question of “what could go wrong” becomes more pertinent than ever. The history of Thalidomide is instructive in this regard.
metamars
@Joe
“I find it axiomatic that if you show me a YouTube video, whatever you’re pointing me to is intellectual garbage at best, and dangerous misinformation at worst.”
Oh, Joe, say it ain’t so!
Here’s a link to a youtube search for “Nobel laureate lectures”: https://www.youtube.com/results?search_query=Nobel+laureate+lectures
Don’t you feel, silly, now?
Guest
I don’t trust Duckworth or any other blue dog, and I suspect this is just a fake compromise to move the discussion away from Medicare for all.
But one nice aspect of lowering the age to 50, besides letting a lot of people retire who need to retire but can’t due to need for insurance, is that 50s are the peak earning years for a big chunk of the popoulation, also when most people start to need a lot more medical care. That would take a big bite out of the market share for the insurers, and if the govt ever got serious about controlling costs, that much more leverage.
I’d call it a big first step, and I would think it would be the hardest segment of the population for the private sector to let go of its death grip on. But like I said, I don’t trust Duckworth. At this point we should be talking about going big to get maximum public support, and she’s trying to go small with something that will just cause lack of enthusiasm and resentment from those left out. Typical centrist Dem.
metamars
Speaking of Nobel laureates, here’s a video of Nobel laureate Luc Mantegnier on his research on the mysterious memory of water: https://www.youtube.com/watch?v=R8VyUsVOic0
metamars
I’ve no idea whether water memory, as investigated by Mantegnier, is related to structured water,. I’ve seen claims that some water devices erase previous memory in the water they produce, but I can’t recall if they’re also claiming their end product is structured water (ala Pollack), and I’ve never seen any evidence for said claim.
The pig headed reaction by the scientific community to Benveniste’s findings (Benveniste being Mantegnier’s predecessor), now independently replicated many times, is yet another sorry example why one should be skeptical of scientific claims of authority. I also view this is an example of mostly an anthropological/tribalistic phenomenon, as opposed to a money related corruption issue.
Then again, there’s this: https://en.wikipedia.org/wiki/Replication_crisis
metamars
$32,500 / year for CBD oil coming? http://www.anh-usa.org/32500-for-cbd-oil/
I’ve seen a video of an epileptic child almost instantly start acting normally, due to CBD oil. CBD oil is very effective in taming brain inflammation.
I don’t trust the US government to give us universal healthcare at a reasonable cost. This isn’t going to happen unless the public organizes, politically, and exerts it’s collective muscle.
When the public gets enough power over the shape and actions of the government that they can dispense with the no bargaining provisions in Medicare Part D, fund FDA approval for no and low profit drugs and medical devices, cap profits for primary care, etc., then at that point it becomes plausible that it can provide universal healthcare coverage in a sustainable fashion.